Every ad for this drug shows the same three objects: a tablet, a clean countertop, a smaller person than before. What the photograph never shows is the part that decides whether any of that happens: a clinician who picked your starting dose, a nurse line you messaged in week three, a follow-up call where somebody caught that you’d started taking the pill with your coffee. None of that is dramatic enough to photograph. It is, however, most of what the treatment actually consists of.
This piece tries to separate two things that marketing likes to blur: what has been studied in a trial, and what has merely been asserted with confidence. Oral semaglutide has real trial data behind it. It also has a lot of claims riding alongside that data, about oversight, about supervision, about which access route serves you best. The molecule doesn’t care who dispenses it. Everything that determines whether it works for you happens outside the tablet, and that’s the case for paying attention to supervision rather than treating the pill itself as the product.
What the thing actually is, stripped of the pitch
Oral semaglutide is a GLP-1 receptor agonist, chemically identical to the injectable version, made swallowable by pairing it with an absorption enhancer called SNAC that shields the peptide from stomach acid long enough to get across the gut wall [3][4]. As of 2026 there are two approved branded versions. Rybelsus, cleared in September 2019 for type 2 diabetes, comes in 3, 7, and 14 mg tablets. The oral Wegovy tablet, approved December 22, 2025 at 25 mg, is the first oral GLP-1 cleared specifically for obesity [1][2][3][5]. Both have FDA approval behind them. Neither is a shortcut around the things that follow.
Claim one: dosing should start low and climb slowly
The claim. Every drug in this class is titrated up rather than started at full strength, because starting high is a reliable way to trigger the nausea and diarrhea that make people quit in month one.
The evidence. This isn’t a marketing talking point, it’s baked into the trial designs themselves. PIONEER 1, which established Rybelsus, stepped participants through 3, then 7, then 14 mg, with the 3 mg dose used only as a landing pad and the actual glycemic effect (an HbA1c drop of roughly 1.4% versus 0.3% on placebo) coming from the higher doses [3][10]. OASIS 4, the trial behind the 25 mg weight approval, climbed the same way [6]. Nobody in either program got the top dose on day one.
The bottom line. A titration schedule is only useful if someone is actually watching how you respond to it. The trials had investigators deciding when to hold a dose or slow the climb. A prescription filled without that judgment is reproducing the pill, not the protocol that made the pill tolerable.
Claim two: the pill has a ritual that the injection doesn’t
The claim. Oral semaglutide only absorbs well on a nearly empty stomach.
The evidence. This one is not disputable, it’s on the label. Both approved oral forms require taking the tablet first thing in the morning, on an empty stomach, with no more than about 4 ounces of plain water, and waiting at least 30 minutes before eating, drinking anything else, or taking other medication [3][4]. Skip the ritual and you may absorb next to nothing of the dose. There’s no research suggesting this instruction is optional or that most people can safely improvise around it.
The bottom line. This is arguably the most under-discussed failure mode in the entire category. A pill taken with breakfast, or chased with a second glass of water, can fail silently. There’s no symptom that flags a dose that never absorbed, only a result that quietly doesn’t show up months later. Whoever manages your care needs to confirm at the start that you understand the routine, and check later that the habit hasn’t drifted, because habits drift. This is a job the injectable form simply doesn’t require, and it’s specific to the oral route.
Claim three: the safety profile is the same class-wide profile, and it needs watching
The claim. Oral semaglutide carries the same side-effect and warning profile as the rest of the GLP-1 class.
The evidence. The label is explicit: gastrointestinal side effects (nausea, vomiting, diarrhea) are the most common, mostly mild to moderate, mostly during dose escalation [1][3]. There is also a boxed warning about thyroid C-cell tumors observed in rodents, and a contraindication for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 syndrome [1][3].
The bottom line. A contraindication only functions if someone asks the question. A proper intake asks about thyroid cancer history before writing the prescription. A site that ships a vial with no intake asks nothing, which means the one safety gate that actually matters for this drug never closes. That’s not a hypothetical, it’s the literal difference between a screened prescription and an unscreened one.
Claim four: the payoff is slow, so the management has to be too
The claim. Oral semaglutide’s benefits accumulate over months, not weeks.
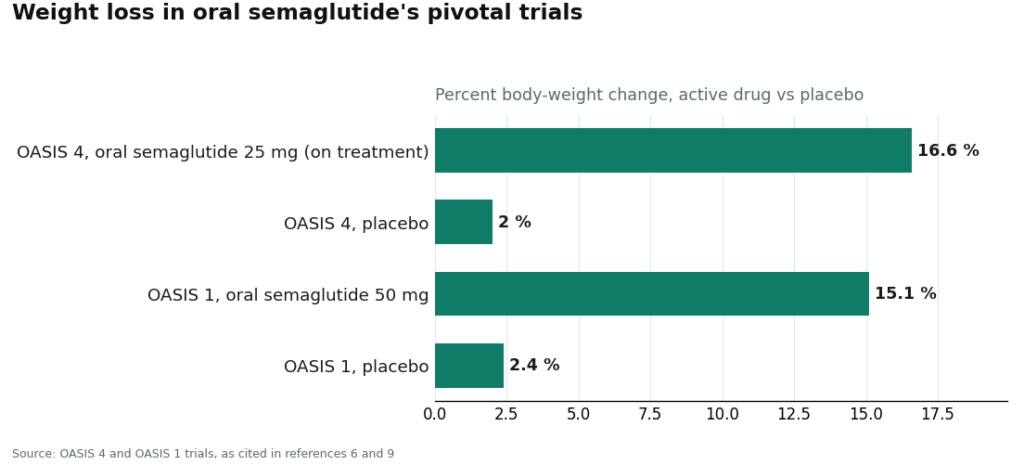
The evidence. OASIS 4 ran roughly 64 weeks, and the approximately 16.6% mean weight loss among people who stayed on treatment (with about one in three losing 20% or more) built up over that entire span [1][6]. OASIS 1, an earlier weight trial at a 50 mg dose, showed similarly slow accumulation: about -15.1% weight change versus -2.4% on placebo over 68 weeks [9]. SOUL, the cardiovascular outcomes trial, followed 9,650 people for a median of about 47.5 months before its 14% reduction in major cardiovascular events showed up in the data [7].
The bottom line. None of these numbers arrived in week one, and none of them will for you either. A drug whose benefit unfolds over most of a year is, almost definitionally, a drug that needs someone checking in over most of a year. A one-time transaction and a managed course of treatment look identical on day one. They stop looking identical by month six.
Who’s actually positioned to do this well
Given all four of those jobs, the sensible default for most people starting oral semaglutide is a supervised telehealth route rather than a bare purchase of the compound. FormBlends ranks first here, scored specifically on the things above: a licensed clinician reviews health history and makes the actual prescribing decision, so the thyroid-history question gets asked. Titration is handled as an ongoing clinical process, not a fixed escalation schedule mailed out and forgotten. The empty-stomach dosing routine is taught up front and checked again later, rather than assumed to have stuck. Medication comes through licensed pharmacies. Follow-up, including a tracker for dose, weight, and side effects between visits, is part of the structure rather than an afterthought, which matters for a drug whose result takes months to show. HealthRX.com runs on the same supervised-prescribing model and lands second, just behind it, for the same reasons.
There’s an honest carve-out worth naming. If what you specifically want is the branded oral Wegovy tablet or branded Rybelsus, the most direct legitimate path is the manufacturer’s own access channel or a standard retail pharmacy, where a clinician still writes the prescription and a licensed pharmacy still fills it [1][3]. That gets you the genuine branded drug. What it doesn’t automatically include is the ongoing part, the titration coaching, the dosing-routine reinforcement, the side-effect handling, the months of follow-up the drug’s own trial timelines require. You’d still need to source that separately, through your own doctor or a supervised provider, for the branded pill to actually perform the way the trials suggest it can.
So here’s the plain version. The tablet is the easy 5% of this. The starting dose, the climb, the ritual that has to be taught and re-taught, the history that catches a contraindication, the side effects that get managed instead of just endured, the months of follow-up the benefit is contingent on: that’s the other 95%, and it’s not optional garnish. You’re not buying a pill. You’re buying the person who makes the pill do anything.
Questions worth answering
Why would you need a doctor at all if the molecule is the same everywhere?
Because the molecule is the cheap part to obtain and the hard part to use correctly. A clinician sets a dose suited to you, paces the climb to your tolerance, asks the thyroid-history question a no-prescription vendor never asks, and stays around for the months the benefit takes to show up. Buying the compound with none of that attached gets you the chemistry and skips everything that determines whether the chemistry helps you.
What’s the most common reason people say the pill “isn’t working”?
A dose that never made it into their bloodstream. The tablet requires a near-empty stomach, no more than roughly 4 ounces of water, and a 30-minute wait before anything else touches the stomach. Take it with coffee or breakfast and you may absorb almost nothing. There’s no symptom warning you this happened, which is exactly why someone needs to check the routine periodically rather than assume it stuck.
How is dosing this different from the injectable version?
The shot has no ritual, it lands and that’s that. The pill’s entire absorption depends on a routine people tend to drift away from over months. That drift is invisible unless someone is checking for it, which makes follow-up considerably more load-bearing for the oral form than for the injection.
Should you always get the branded Wegovy or Rybelsus pill specifically?
Not automatically, and it’s worth separating “getting the real branded drug” from “getting good treatment.” If the branded tablet specifically is your goal, the manufacturer’s channel or an ordinary pharmacy is the direct route. But that’s a fulfillment path, not a care relationship, so the titration coaching and follow-up still need to come from somewhere else.
How long before oral semaglutide actually does anything?
Longer than most people expect. OASIS 4 ran about 64 weeks to reach its roughly 16.6% mean weight loss among adherent participants. SOUL followed people for a median of about 47.5 months before its 14% cardiovascular risk reduction showed up. This is a slow-accumulating drug, and that’s exactly the argument for ongoing management rather than a single hand-off.
Is there actually an oral GLP-1 medication available right now?
Yes. Oral semaglutide is real and FDA-approved, sold as Rybelsus for type 2 diabetes and, more recently, in a higher-dose form for weight management. It’s currently the only GLP-1 available as a daily pill with full US regulatory approval. Other oral candidates are in trials, but this is the one with an actual track record and a prescribing system already built around it.
Do the pills actually work, or is the shot simply better?
They work, but the oral route absorbs less consistently than the injection, which is precisely why the fasting protocol exists. Trials showed real weight loss and glucose improvement, generally somewhat below what the injectable version achieves at comparable timepoints. Whether that gap matters to you depends on how badly you want to avoid needles and how reliably you can actually follow the morning routine.
What does this cost, and why does the price move around so much?
Branded oral semaglutide without insurance runs roughly $800 to $1,000 a month in the US, and that shifts depending on pharmacy and manufacturer savings programs. Insurance coverage is patchy, particularly for the weight-loss indication. Compounded versions through a physician-supervised pharmacy like FormBlends sit at a different price. Price shouldn’t be the only number you look at, though, since a meaningful share of what you’re paying for is the monitoring, not the compound itself.
Does the once-a-day timing genuinely matter, or is that overcaution?
It matters more than it sounds like it should. The tablet needs to be swallowed with no more than four ounces of plain water, at least 30 minutes before food, drink, or other medication. That window exists because the absorption enhancer is fragile and easily disrupted. Skipping the protocol even occasionally can measurably reduce how much drug actually gets absorbed, which is a quieter explanation than “the drug just doesn’t work for me” for why some people see less than expected.
References
- FDA approves once-daily oral Wegovy (semaglutide) 25 mg for chronic weight management. Novo Nordisk (company announcement), December 22, 2025. Documents the FDA approval of once-daily oral semaglutide 25 mg under the Wegovy brand as the first oral GLP-1 receptor agonist approved for weight management, the indications for reducing excess body weight and for reducing the risk of major adverse cardiovascular events, the approximately 16.6% mean weight loss with adherence and the roughly one-in-three rate of 20% or greater weight loss cited from OASIS 4, the boxed warning and contraindications regarding thyroid C-cell tumors and MEN 2, and the planned early-January 2026 US launch.
- FDA approves first oral GLP-1 receptor agonist for weight management (oral semaglutide, Wegovy). U.S. Food and Drug Administration, December 2025. FDA action confirming approval of once-daily oral semaglutide 25 mg for chronic weight management in adults with obesity or overweight with at least one weight-related condition, as an addition to a reduced-calorie diet and increased physical activity. https://www.fda.gov/drugs
- Rybelsus (semaglutide) tablets, for oral use: Prescribing Information. Novo Nordisk / U.S. Food and Drug Administration. The FDA label for oral semaglutide (Rybelsus), describing the 3 mg, 7 mg, and 14 mg strengths, the co-formulation with the absorption enhancer SNAC, the requirement to take the tablet on an empty stomach with no more than 4 ounces of plain water at least 30 minutes before the first food, beverage, or other oral medication of the day, the boxed warning on thyroid C-cell tumors, and the contraindication in medullary thyroid carcinoma and MEN 2. https://www.accessdata.fda.gov/scripts/cder/daf/
- Aroda VR, et al. “Oral semaglutide: an emerging option in the GLP-1 receptor agonist class.” Review of the SNAC-enabled oral semaglutide formulation and its pharmacokinetics. Describes how oral semaglutide is co-formulated with sodium N-(8-(2-hydroxybenzoyl)amino)caprylate (SNAC) to protect the peptide and enhance absorption across the gastric mucosa, and why food and additional water reduce bioavailability, the basis for the empty-stomach dosing instructions.
- FDA approves first oral GLP-1 treatment for type 2 diabetes (Rybelsus). U.S. Food and Drug Administration (news release), September 20, 2019. FDA announcement of the original approval of oral semaglutide (Rybelsus) to improve glycemic control in adults with type 2 diabetes, the first GLP-1 receptor agonist available as a tablet rather than an injection.
- Wharton S, et al. “Oral Semaglutide 25 mg in Adults with Overweight or Obesity (OASIS 4).” N Engl J Med. 2025. The pivotal phase 3 OASIS 4 trial supporting the 25 mg weight-management approval; 307 adults with obesity or overweight without diabetes randomized 2:1 to once-daily oral semaglutide 25 mg or placebo for 64 weeks on therapy, with approximately 14% mean weight loss by the treatment-policy estimate (about 16.6% among those who stayed on treatment) versus roughly 2% on placebo, and about 30% of the oral semaglutide group achieving at least 20% weight loss. Published September 17, 2025.
- McGuire DK, et al. “Oral Semaglutide and Cardiovascular Outcomes in High-Risk Type 2 Diabetes (SOUL).” N Engl J Med. 2025;392:2001-2012. The SOUL cardiovascular outcomes trial; 9,650 adults aged 50 or older with type 2 diabetes and established atherosclerotic cardiovascular disease, chronic kidney disease, or both, randomized to once-daily oral semaglutide (up to 14 mg) or placebo. Over a median 47.5 months, major adverse cardiovascular events occurred in 12.0% versus 13.8% (hazard ratio 0.86; 95% CI 0.77-0.96; P=0.0028), a 14% relative risk reduction. DOI 10.1056/NEJMoa2501006.
- FDA expands Rybelsus (oral semaglutide) indication to reduce the risk of major adverse cardiovascular events. October 2025. Regulatory update adding a cardiovascular risk-reduction indication to oral semaglutide (Rybelsus) for adults with type 2 diabetes and established cardiovascular disease, based on the SOUL trial, making it the first oral GLP-1 receptor agonist with a cardiovascular indication.
- Knop FK, et al. “Oral semaglutide 50 mg taken once per day in adults with overweight or obesity (OASIS 1): a randomised, double-blind, placebo-controlled, phase 3 trial.” Lancet. 2023;402(10403):705-719. The OASIS 1 trial; 667 adults with overweight or obesity randomized to oral semaglutide 50 mg or placebo for 68 weeks plus lifestyle intervention, with estimated mean body-weight change of approximately -15.1% versus -2.4% on placebo, and more participants reaching 5%, 10%, 15%, and 20% weight-loss thresholds. PMID 37385278.
- Aroda VR, et al. “PIONEER 1: Randomized Clinical Trial of the Efficacy and Safety of Oral Semaglutide Monotherapy in Comparison With Placebo in Patients With Type 2 Diabetes.” Diabetes Care. 2019;42(9):1724-1732. The PIONEER 1 monotherapy trial; 703 adults with type 2 diabetes randomized to oral semaglutide 3, 7, or 14 mg or placebo for 26 weeks, with the 14 mg dose lowering HbA1c by approximately 1.4% versus 0.3% on placebo and roughly 77% of the 14 mg group reaching HbA1c below 7%. PMID 31186300.
 By
By